Increasingly, individuals are coming to us with histamine-associated conditions. It is therefore of particular concern to me to inform about this topic. The reason for this increase is ultimately not fully clear, but the increase and diversity of symptoms is pronounced and without a doubt.
We are seeing an increased frequency of mast cell activation syndrome (MCAS) following coronavirus infections and also following coronavirus vaccinations as part of a POST VAC syndrome. Although MCAS is a medical condition recognized in the field of medicine, it is often not well understood in traditional outpatient and inpatient DRG medicine (a DRG code is assigned to each diagnosis with an optimal length of stay for optimal reimbursement). There is a widespread lack of knowledge and patients are often stigmatized as having a mental illness.
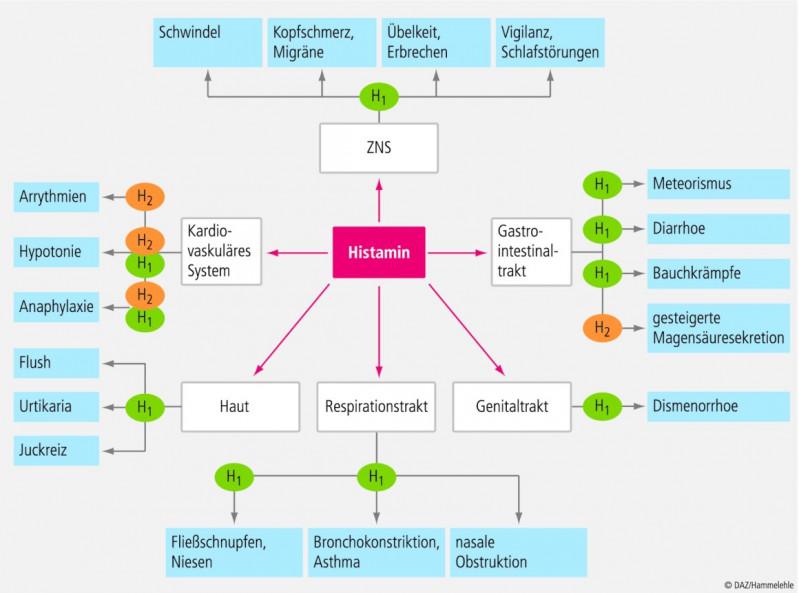
We now want to examine different presentation patterns of symptoms associated with histamine, as shown in the following graphic. The diagram below shows histamine-associated complaints, broadly simplified, through H-1 and H-2 histamine receptors.
Differentially, we clarify histamine degradation disorders, an increased formation of histamine in the intestine as well as a mast cell activation syndrome or a mastocytosis (the latter is very rarely present).
A histamine intolerance or impaired histamine degradation can be primarily or secondarily caused (primarily = genetically / HNMT or DAO polymorphisms or secondarily due to a coenzyme deficiency: zinc, copper, and/or vitamin B-6 deficiency or damage to the small intestine mucosa, which functions as a production site for 50-70% of DAO).
It is important to differentiate between a secondary (reversible) and primary form of histamine intolerance.
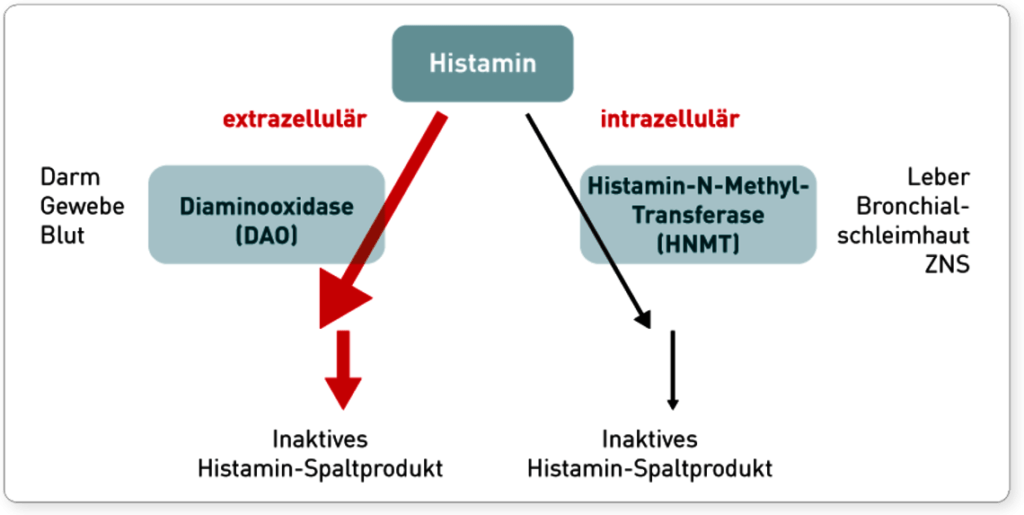
In the primary form, there are genetic changes in the histamine-degrading enzymes (DAO and HNMT). Diamine oxidase (=DAO) is responsible for the degradation of histamine in the intestine and extracellularly. However, DAO does not only degrade histamine, but also histamine-like substances, the biogenic amines. This group includes tyramine, putrescine, cadaverine and octopamine. These can themselves also play a role in a variety of medical conditions (e.g. autism, headaches, etc.). A look at the intestinal flora is therefore always recommended, even in the lack of intestinal symptoms, since these substances are formed by certain intestinal germs (see below) and, for example, in the case of a simultaneously present Leaky Gut Syndrome, they enter the blood system and develop their effect in the body.
The histamine N-methyltransferase (=HNMT) has the task of breaking down histamine in the body, e.g. in the brain. For both genes there are known polymorphisms, which can lead to a degradation disorder.
Most of the time, degradation disorders are secondary or, despite the presence of polymorphisms, it is usually possible to optimize histamine degradation through various therapeutic measures.The following graphic shows the degradation of histamine (courtesy of IMD Berlin).